Expression of aquaporin channels 1 and 5 during mechanical ventilation
 Gustavo Fabregat
Gustavo Fabregat2010, European Journal of Anaesthesiology
Sign up for access to the world's latest research
AI-generated Abstract
This study investigates the expression of aquaporin channels 1 and 5 during mechanical ventilation, focusing on their roles in fluid homeostasis and cellular responses in the lungs. The research highlights changes in the levels of these channels under various mechanical ventilation settings, contributing to our understanding of ventilatory impact on pulmonary function and the potential for targeting aquaporins in therapeutic strategies.
Figures (435)



















![Materials and Methods: After suffering two cases of possible reactions in operating room. We review what has been done retrospectively and the it- erature, we found gaps in the diagnostic phase that generated an increase in avoidable costs, so we set contact the Allergy Service of our hospital, result of this collaboration is this article and following algorithm. Results and Discussion: As a guideline the Community of Castilla la Mancha sets prices for specialized medical tests, diagnosis and treatment in the first consultation by 185.22 euros and 69.42 euros in successives. [8]. These patients have an average of three consultations of allergy to the final diagnosis. If we stick to our hospital surgical activity in 2005: 44.367 events, applying the percentages of the introduction there would be 3 “true” allergic reactions which require monitoring by the Department of Allergy and 30 cases of anaphylactoid reaction in which an initial determination of tryptase would have saved 9721.8 euros to the hospital.](https://figures.academia-assets.com/48316896/figure_011.jpg)




























![Values are expressed as number of patients (%). CRO: complete response(CR) of PACU 1 min, CR1: CR of postoperative 1hr CR2: CR of postoperative 2hr CR6: CR of postoperative 6hr CR24: CR of POD 1 CR48: CR of POD 2, No vomiting 24: no vomiting 0-24h after surgery, tP < 0.05, compared with control group. [table2]Percent of complete response and proportion of no vomiting](https://figures.academia-assets.com/48316896/table_028.jpg)

















































![aN Se a a ee ee EE ee aS ae ee and were randomly assigned to receive either balanced xenon or sevoflurane anaesthe- sia with remifentanil titrated to clinical needs. BIS monitoring was blinded to the perform- ing anaesthetist and values were continuously assessed by accessory study personnel. Results and Discussion: 30 patients were enrolled in each group, comparable in respect to age, gender, height, ASA status, baseline systolic blood pressure anc baseline heart rate. BIS values during induction and maintenance of xenon anaesthe- sia correlated well with the value range recommended for deep hypnosis and with val- ues obtained during sevoflurane anaesthesia.Bispectral Index monitoring thoroughly indicated an adequate level of hypnosis during balanced xenon anaesthesia guidec according to clinical parameters. Controversial results obtained from former studies [2] indicating unpredictable influences of xenon on the BIS were not confirmed.](https://figures.academia-assets.com/48316896/figure_051.jpg)







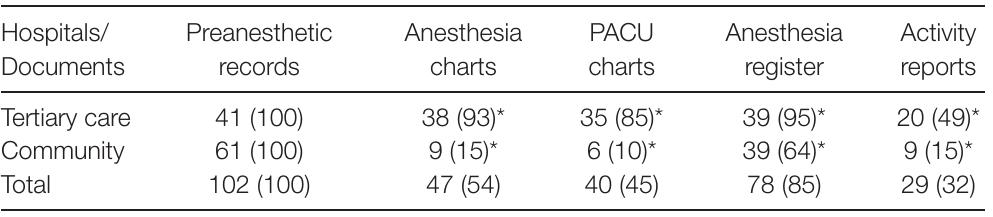
![Daca cts Figure 2. Steady-state detection results for one patient outside the training set. From top to bottom: drug's effect-site concentration targets and arithmetic rule DIF; filtered BIS, filtered mean blood pressure and filtered ECG heart rate with the input steady-state periods overlapping; combined measure of output steady-state. Results and Discussion: 22 patients, 12 men, 55.9+13.0 years, 69.3413.4kg and 164.346.9cm. Fig. 2 presents the results for one patient outside the training set, with the inputs SS detection followed by the filtered signals (BIS, ECG heart rate and blood pressure) and combined measure of SS. The performance of the method was visually evaluated, with the results indicating an adequate detection of the SS periods. We also observe that SS in the inputs is not always followed by SS in the output signal [4], this may be the result of external interferences not only related to the input drugs.](https://figures.academia-assets.com/48316896/figure_056.jpg)
![Figure 1. Diagram presenting the algorithm steps: the patient is the system, with propofol and remifentanil drugs effect-site concentrations (Cc) as inputs, and mean blood pressure (MBP), ECG heart rate (HR) and BIS as measurable outputs. On top we have the steady- state detection arithmetic rule for the inputs, and on bottom we have the wavelet based algorithm summary to determine the combined steady-state index. Materials and Methods: Data collected every 5 s (Rugloopll) during 22 urologi- cal procedures under TCI of propofol and remifentanil (Gchnider [1] and Minto’s [2] PkPd models). Data from 5 patients used to extract periods of SS by visual analysis, and tuning parameters for the wavelet detector [4]. The tuned algorithm was applied to all patients. Drugs SS periods were identified by an arithmetic rule. Fig. 1 summa- rizes the algorithm. The SS index varies from O (non-SS) to 1 (SS), with smoothing period of 15s. MATLAB R2007a was used for signal analysis.(Data: Mean+SD)](https://figures.academia-assets.com/48316896/figure_057.jpg)





















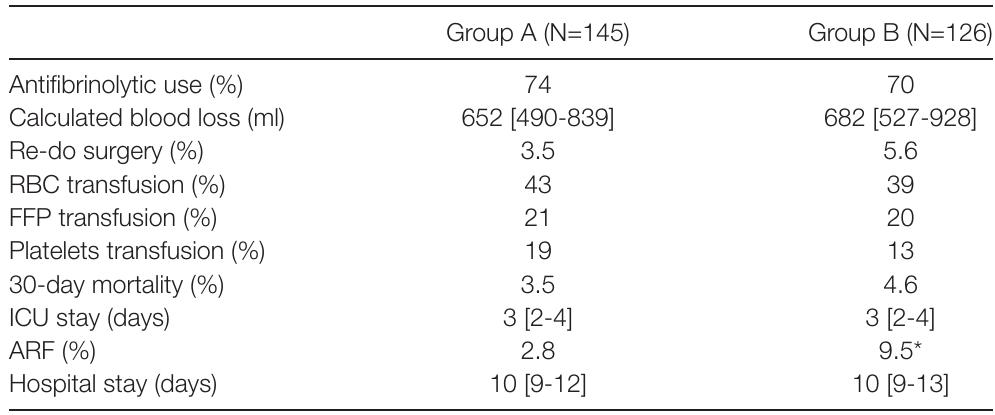
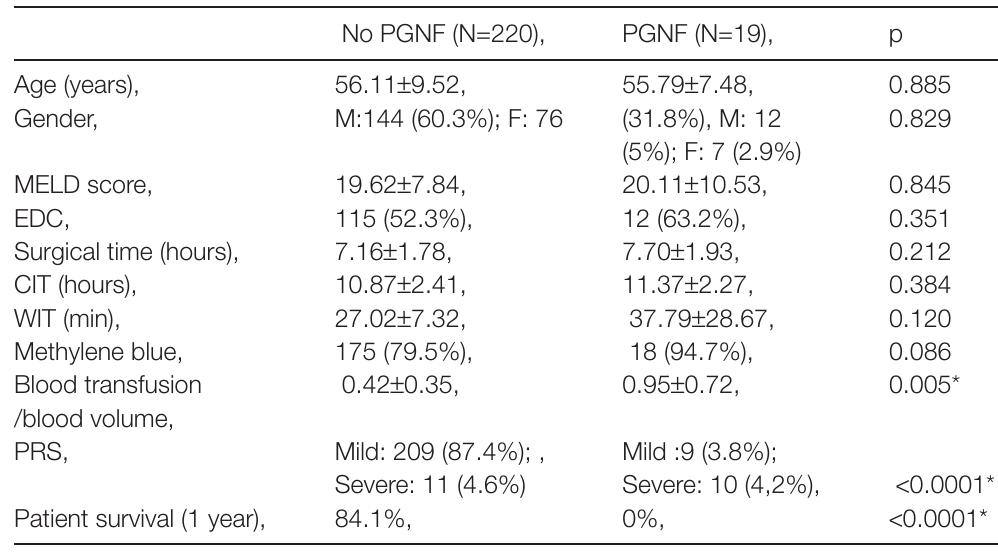
![Figure2. Kaplan-Meier Survival Analysis of Patients with normal and elevated Postoperative Troponin I. Results and Discussion: Findings: Of 378 patients, who underwent major head and neck cancer surgery, 57 patients (15%) developed an elevated Tnl; 90% of which occurred within the first 24 hours after surgery. Pre-existing renal insufficiency (unadjusted OR [OR]: 4.60, 95% Cl 1.53-13.82), coronary artery disease (OR: 2.33, 95% Cl 1.21-4.50), peripheral vascular disease (OR: 2.83, 95%Cl 1.31-6.14), hypertension (OR: 2.22, 95% Cl 1.20-4.12), and previous combined chemotherapy and radiation (OR: 2.68, 95% Cl 1.04-6.91) were asso- ciated with elevated postoperative TnI. Patients with elevated Tnl had a signifi- cantly longer length of stay in the hospital (8.5 vs. 10.1 days; p= 0.014) and ICU (8 vs. 4.5 days; p= 0.001) and an 8-fold increased risk of death at 60 days after surgery (OR 7.62; 95% Cl 1.98 — 29.31). At one year, patients with an abnormal postoperative Tnl were twice as likely to die (OR 1.93; 95% Cl 1.02 — 3.63).](https://figures.academia-assets.com/48316896/figure_071.jpg)



















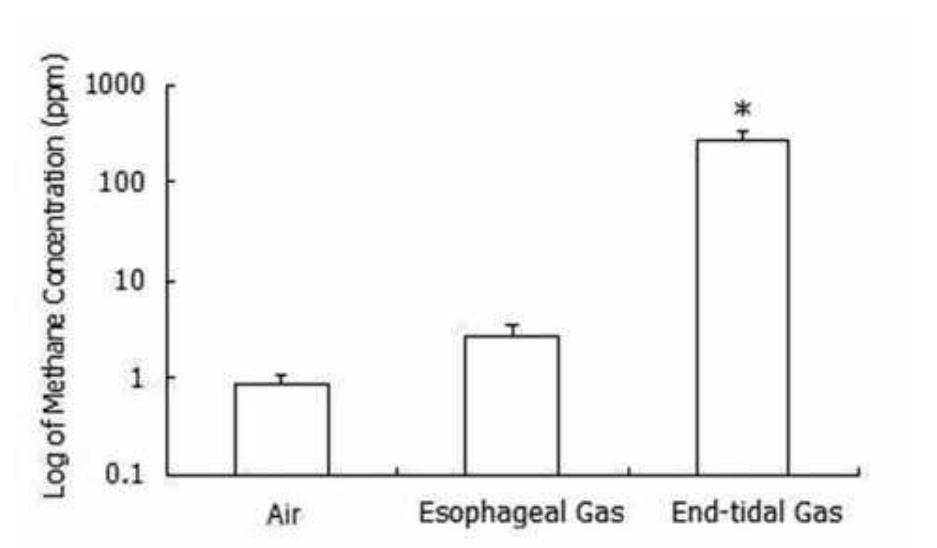
![Respiratory parameters during both periods (n=82) Conclusion(s): During OLV, PEP does not maintain oxygenation when V, is reduced. Lowering Vt might be efficient in reducing lung injury but the use o' such protocol may require the acceptance of possibly lower PaO, and alveolar ventilation. Results and Discussion: ]V, = tidal volume, RR = respiratory rate, Pplateau = end inspiratory plateau pressure, PEEP = positive end expiratory pressure, Pmean = mean alveolar pressure, Pe,CO, = end tidal CO,, PaCO, = arterial carbon dioxide tension, PaO, = arterial oxygen tension, SAP=Systolic arterial pressure. HR = Hear Rate. The PaO,/FiO, ratio significantly decreased during low Vt ventilation (mean difference = -18.8; 95% IC [-34.0 to -3.5], P=0.02). Any significant increase of intrinsic PEEP has been observed between both groups.](https://figures.academia-assets.com/48316896/table_072.jpg)

















































![Figure Arteriovenous fistula occlusion rates 6-weeks and 3-months after surgery. Data expressed as percentage of patients GA, general anesthesia, RA, regional anesthesia, LA, local anesthesia GA, general anesthesia; RA, regional anesthesia; LA, local anesthesia; LOS, length of stay. Data expressed either as mean + SD, median [range], or number of patients (%).](https://figures.academia-assets.com/48316896/figure_104.jpg)







































![Data = https://www.academia.edu/28010776/effect site concentrations of Propofol (mean + SD (ug/ml); * P<0.05 as compared to saline Table 1. Effect of Clonidine on Propofol requirements haemodynamics were aicilar in both groups. Effect site concentrations of PROP [table 1] and REMI [table 2] were significantly less in clonidine group (respectively P=0.029 et P=0.05).](https://figures.academia-assets.com/48316896/table_119.jpg)





















![Results and Discussion: Six patients were identified,all of whom had some form of neuraxial blockade. Table 2 shows the risk factors for each patient. [table1]Many of these risk factors relate to being in labour itself but when com- bined with neuraxial blockade,surgery or a critical care stay,parturients are at high risk of developing pressure ulcers.](https://figures.academia-assets.com/48316896/table_135.jpg)









![Results [All data presented as median (lQR)]](https://figures.academia-assets.com/48316896/table_141.jpg)
















































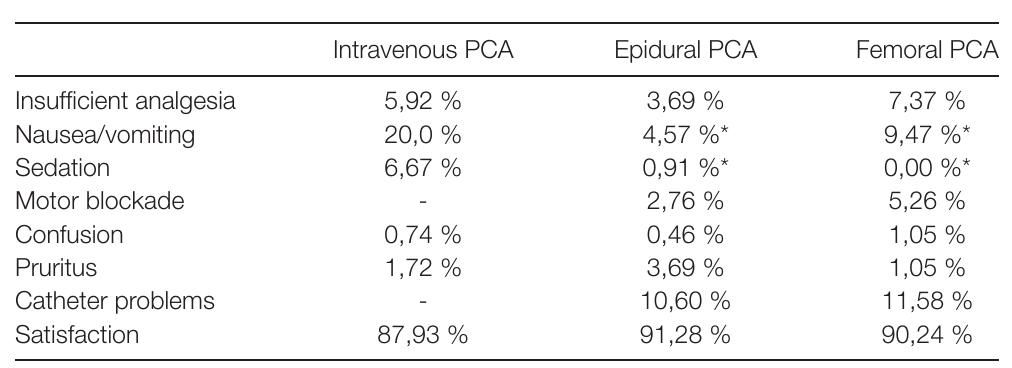
![Results and Discussion: 135 patients received in the postoperative period intravenous patient-controlled analgesia (PCA) with morfine, 217 epidural PCA and 95 femoral nerve PCA. Following pain scores (numeric rating scale) were observed: Following complications, adverse effects and patient satisfaction were observed:[table2]Patients with epidural and femoral nerve PCA had lower pain scores on movement 24 and 48 hours postoperatively and less nausea/ vomiting and sedation than patients with intravenous PCA with morfine.](https://figures.academia-assets.com/48316896/table_166.jpg)






















![Conclusion(s): Performance of electrostatic filters in the clinical setting may not be worse than pleated filters. Factors other than patient contamination levels Results and Discussion: 8/86 (9%) filters had excessive contamination on the machine side. However, only one of these was also contaminated on the patient side. Previous studies have mainly shown contamination on the machine side if it also occurred on the patient side. Lower levels of contamination on the machine side were observed in the current study compared to previous testing of electrostatic filters (9% versus 13%) [ref 2]. However, previous data for electrostatic filters was from a paediatric population where patient side con- tamination levels were higher. There did not appear to be a significant difference in ‘failure rate’ between the small electrostatic filter in this study and a pleated filter in a previous study (8% vs 9%) [ref 2].](https://figures.academia-assets.com/48316896/table_179.jpg)












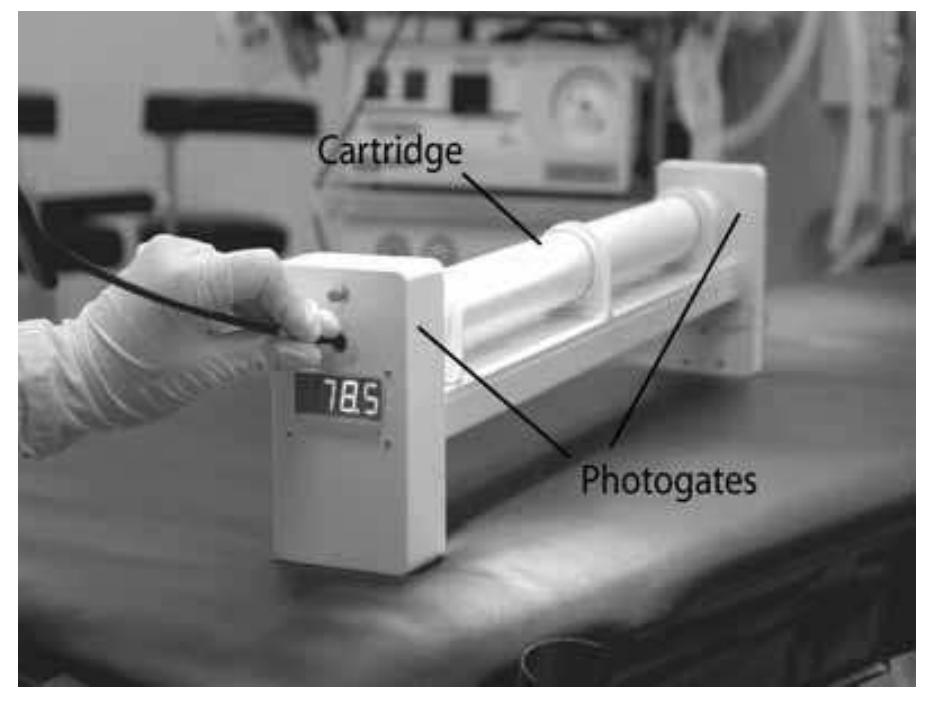
![Conclusion(s): EVA proved to be efficient in restoring oxygenation quickly and limiting hypercarbia over a period of 15 minutes through a 2 mm transtracheal catheter in hypoxic pigs with a completely obstructed upper airway. Results and Discussion: The minute volume necessary to maintain nor- moventilation during IPPV was 9.9 [9.1-12.0] L/min. After 2 minutes of apnea EVA restored oxygenation within 10 seconds.](https://figures.academia-assets.com/48316896/table_183.jpg)




![*responders chose one or more options. Conclusion(s): The findings of this survey suggest that the majority of units use DLT as the method of lung isolation. This may be related to the well docu- mented advantages of DLT over BB [1]. Our findings suggest that gender and height are most likely to be used to predict DLT size. Although the CXR tracheal diameter is more predictive [2], it was the least used criteria. When managing an unpredicted difficult airway, 73% of units used tracheal tube introducer to guide DLT insertion. Caution is advised when this technique is used as the Frova, cur- rent gold standard single-use introducer, is not recommended for use with DLT. When confirming DLT position, 7.7% of units use clinical examination, 19.2% of units use fibreoptic scope and 73% of the units use both methods. Fibreoptic confirmation is recommended given the anatomical variations in the tracheo- bronchial tree and the adverse complications of a misplaced DLT. Dafavenmnnanc:](https://figures.academia-assets.com/48316896/table_186.jpg)












![VATS, video-assisted thoracoscopy; (n), number of patients Materials and Methods: We selected 22 ASA I-Il patients (without predicted difficult airway management and with normal pulmonary function tests [FVC> 80% and FEV1 > 80% predicted]) undergoing different thoracic surgery proce- dures in which one lug ventilation was necessary. Lung isolation was achieved introducing the bronquial blocker through the I|-GEL supraglottic device under direct flexible fibrobroncoscopic vision.](https://figures.academia-assets.com/48316896/table_195.jpg)




![Abstract 19AP6-1 — Impulse, Peak Force and Time to Intubation with GVL in Four Manikins Data expressed as median [IQR], N=Newton, s=seconc](https://figures.academia-assets.com/48316896/table_197.jpg)








![Data expressed as median [IQR]. Impulse (Newtons/second). Peak Force (Newtons). A=Laerdal®SimMan, B=Trucorp AirSim™™Advance, C=Laerdal@Airway Management Trainer, D=Ambu®Airway Man. Impulse and Peak Force with MDL and GVL](https://figures.academia-assets.com/48316896/table_202.jpg)