 Johnny Pujols
Johnny PujolsAbstract
I would like to dedicate this book to my family for all their support and encouragement despite the endless evenings and weekends spent on this book. A special thanks to my wife, Mala who created some of the initial anatomical drawing for this book.
Figures (631)

































































































































































































































































































































































![Fig. 8.8] Ultrasound image of the azygos vein at a lower level draining into the superior vena cava.](https://figures.academia-assets.com/41150239/figure_373.jpg)
























































































































































































































































Key takeaways
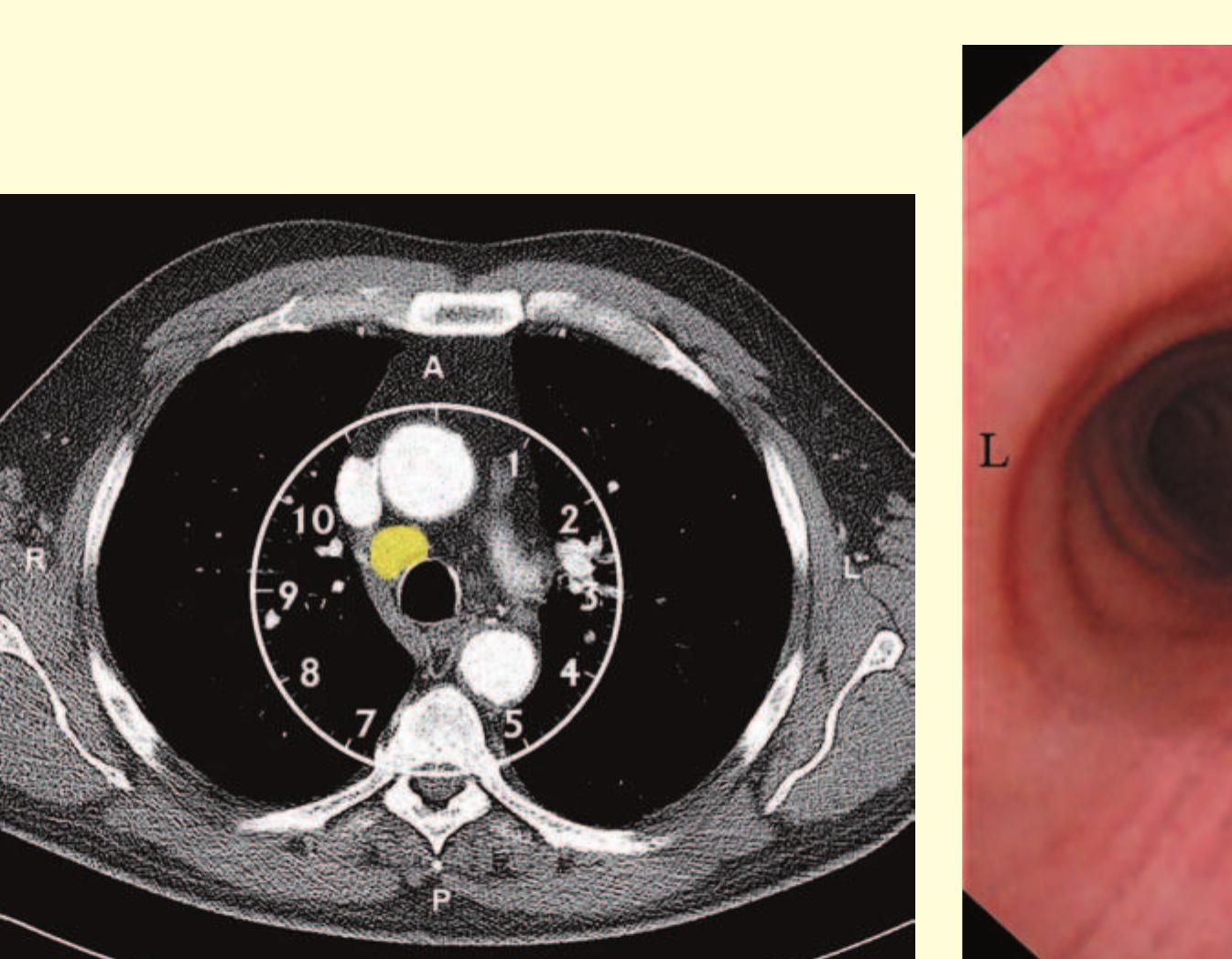
- The bronchoscope is then rotated anticlockwise by 150° to examine the subcarinal lymph nodes (station 7), extending down to the distal margin of the bronchus intermedius.
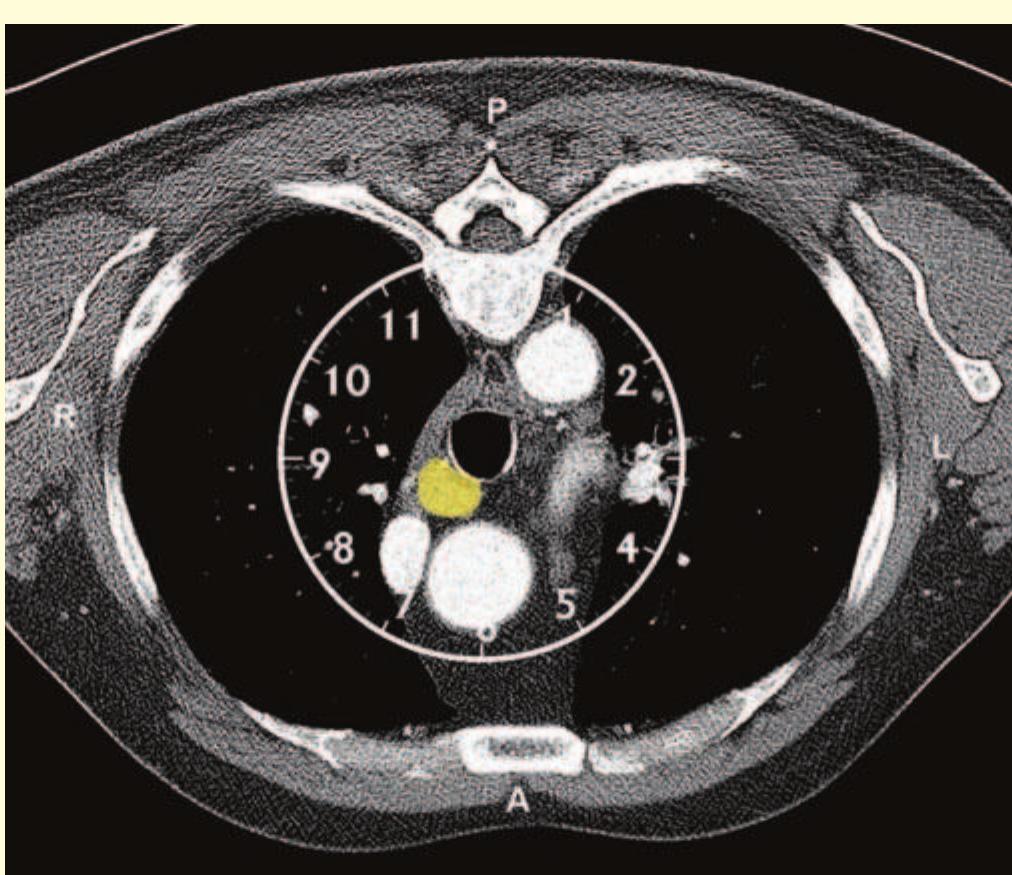
- Superior to the 11R lymph node, the right upper lobe bronchus and pulmonary artery may be visible.
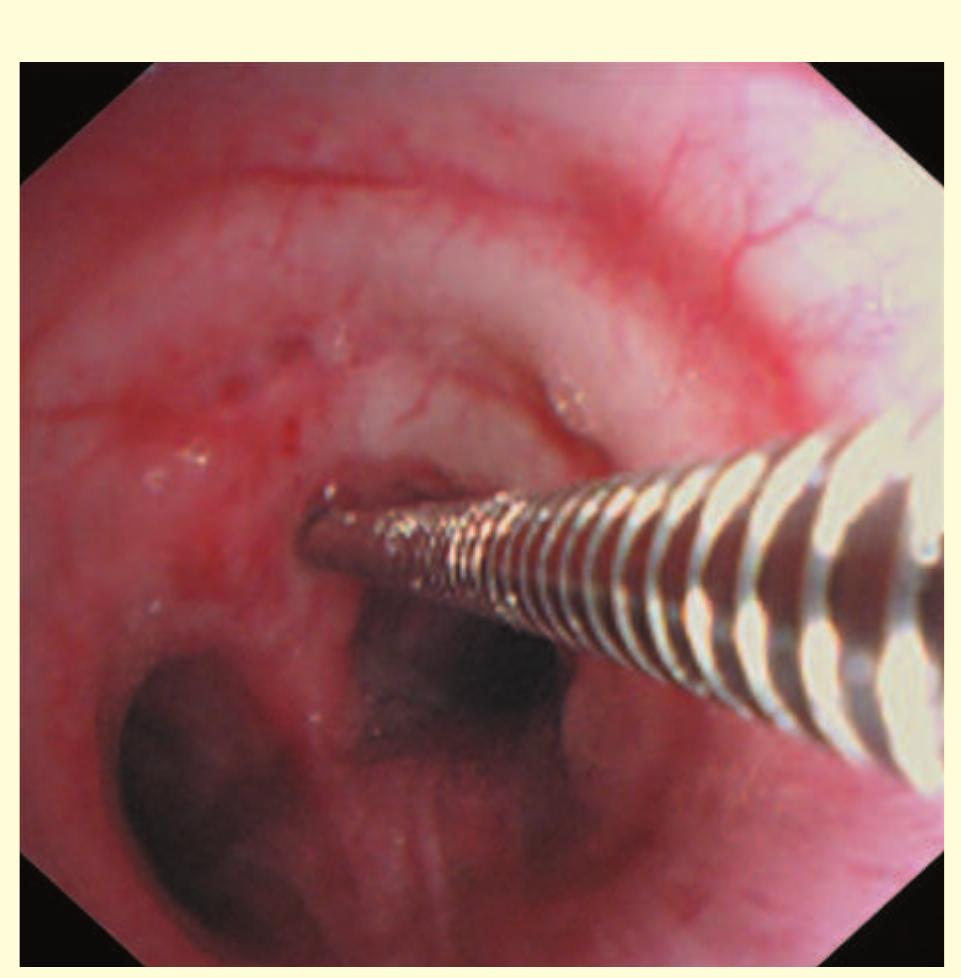
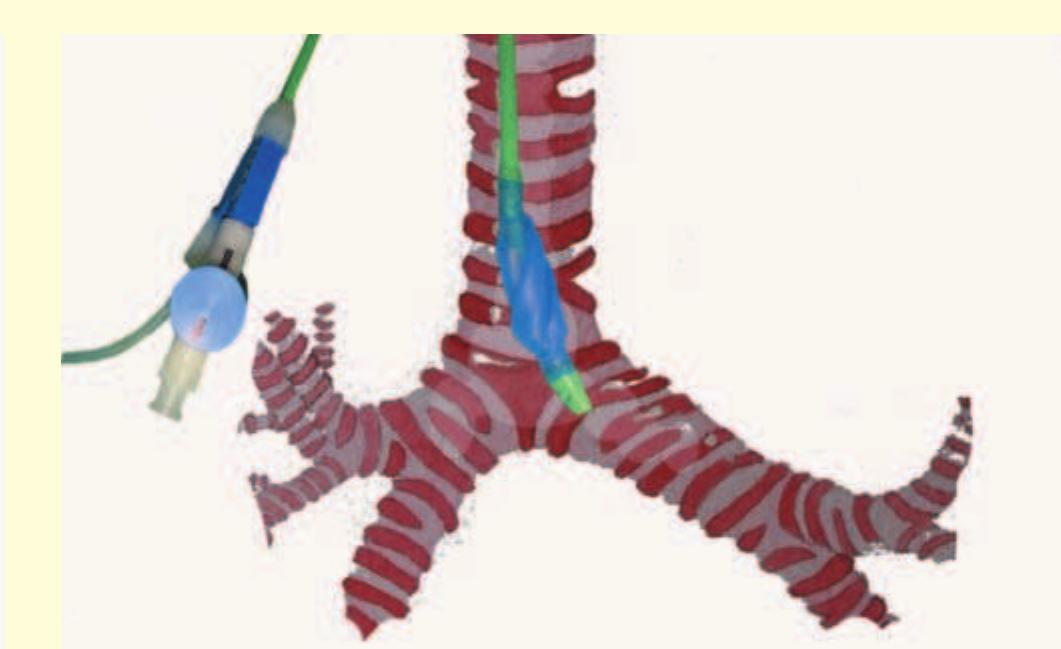
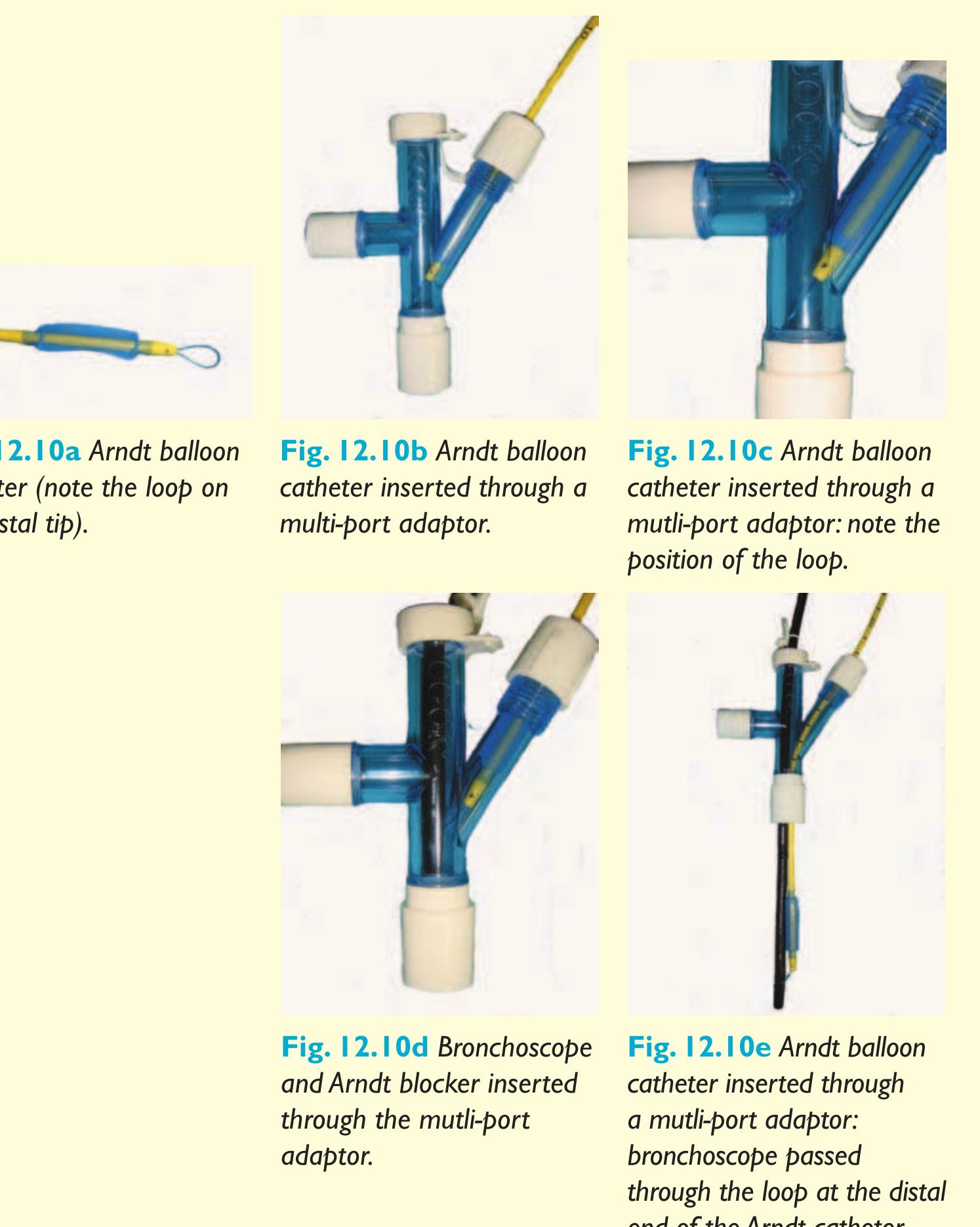
- Once the loop is tightened around the bronchoscope, the endobronchial blocker can be guided to any lobar bronchus (Fig. 12.11).
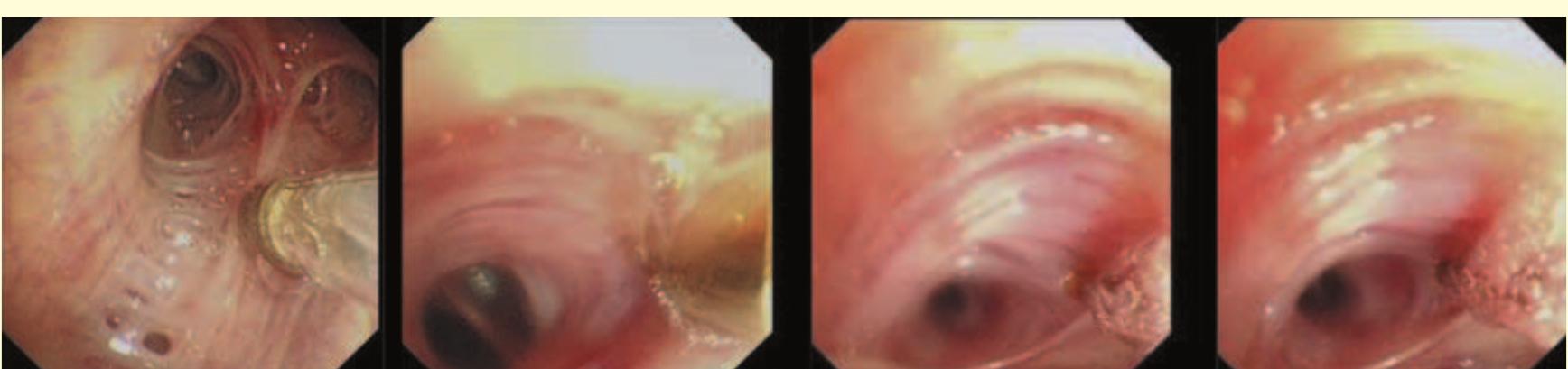
- Bronchoscopy with the nasal approach is performed and a polyethylene catheter is placed through the instrument channel of the bronchoscope and into the desired airway.
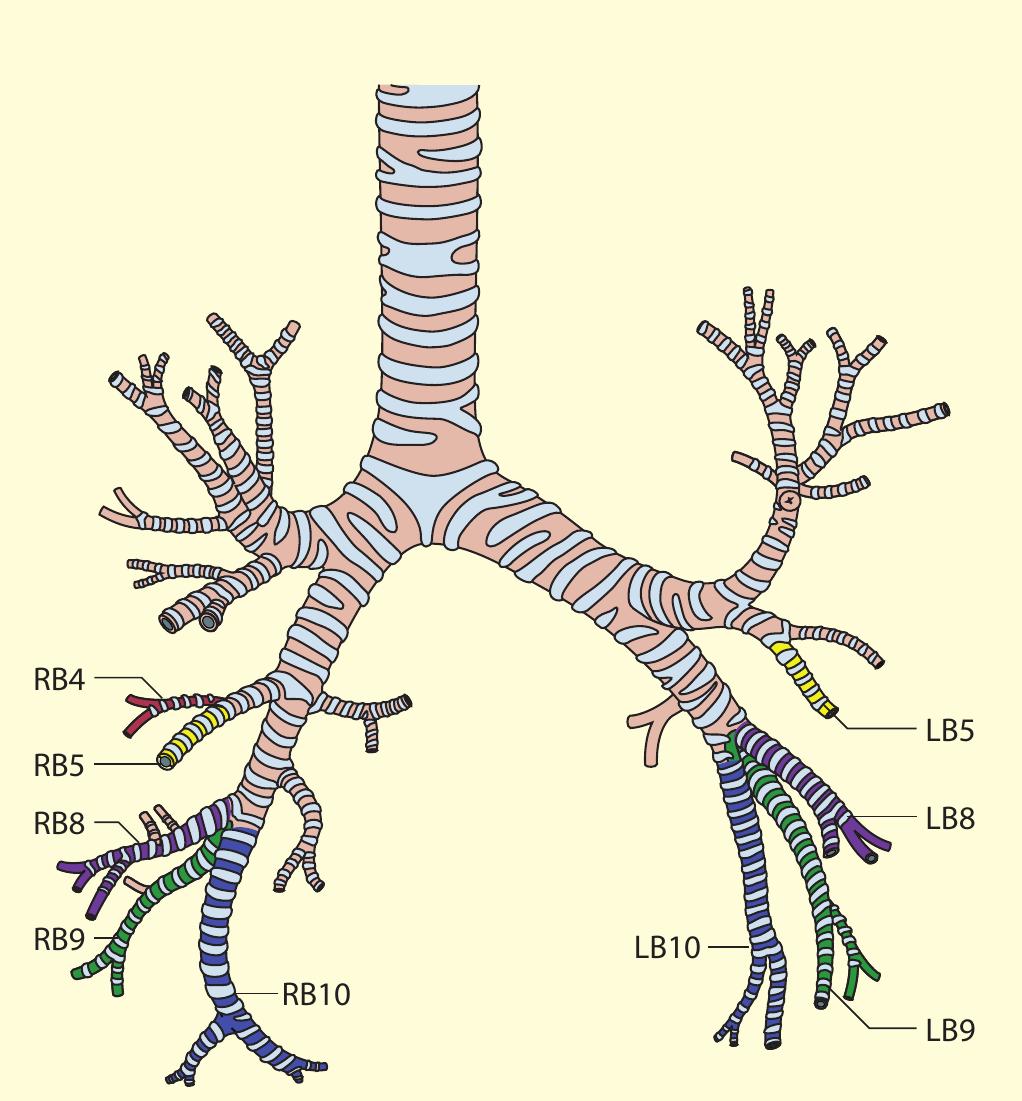
- Our approach, for example, for the right lower lobe is to treat RB10 (right posterior basal bronchus) first, using the BF260 bronchoscope (external diameter 4.3 mm) so that the distal subsegments can be assessed.
